
Ageing is not neutral - a new FemTechnology Report on Longevity
Sex differences shape how we age, yet most longevity research still treats them as peripheral.

Longevity is having a mainstream moment. Aging clocks, senolytics, mitochondrial rejuvenation, precision health. The conversation is expanding fast. Yet one assumption still sits underneath most models of aging: that the biology being measured is universal.
It is not.
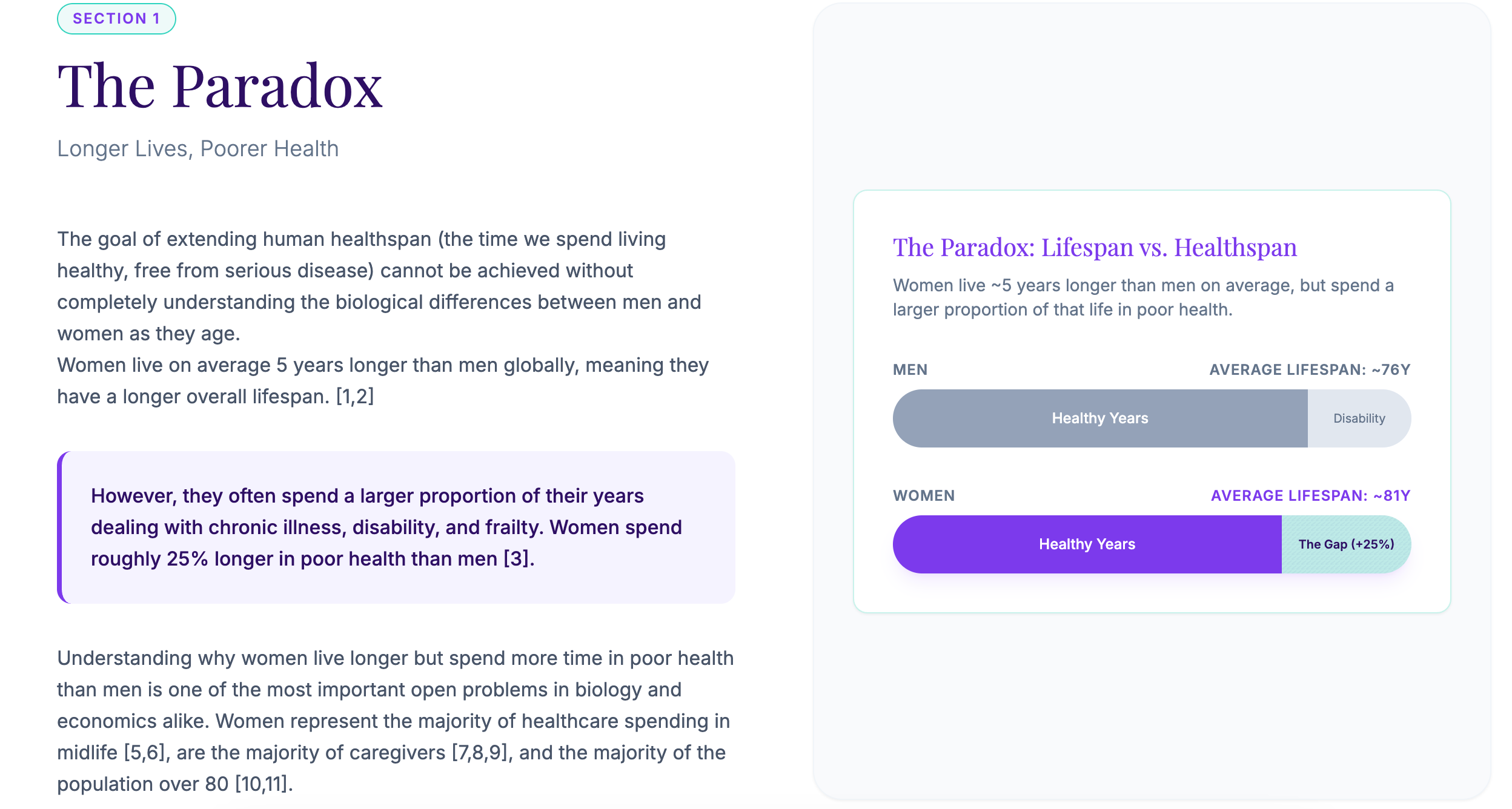
Men and women age differently. The data is clear. Women live longer. Women spend significantly more of those additional years in poor health. On average, women add about 5 extra years of life yet experience about 25% more time with disability or chronic disease.
If longevity science is going to evolve from hype to impact, sex-based differences can’t remain an afterthought.
That’s why we created the report The Missing Half of Longevity Science, a concise, evidence-grounded overview of where biology diverges, where research falls short, and what needs to change to build interventions that work for everyone.
This gap is not only a clinical problem. It is also an economic one. Women account for the majority of midlife healthcare spending. Women provide most unpaid care. Women make up the majority of the population over eighty. These numbers shape workforce participation, pension strain, national health expenditures, and longevity investment strategies. You can read more about in our other FemTechnology Reports.
The paradox is now unavoidable. A longer lifespan does not equal a longer healthspan.
A Missing Variable in the Longevity Toolkit
Most longevity trials and mechanistic aging research still rely on male subjects. In one systematic review of pharmacological lifespan studies in mice, 40% used only males or did not report sex. When both sexes were included, 73% of results diverged.
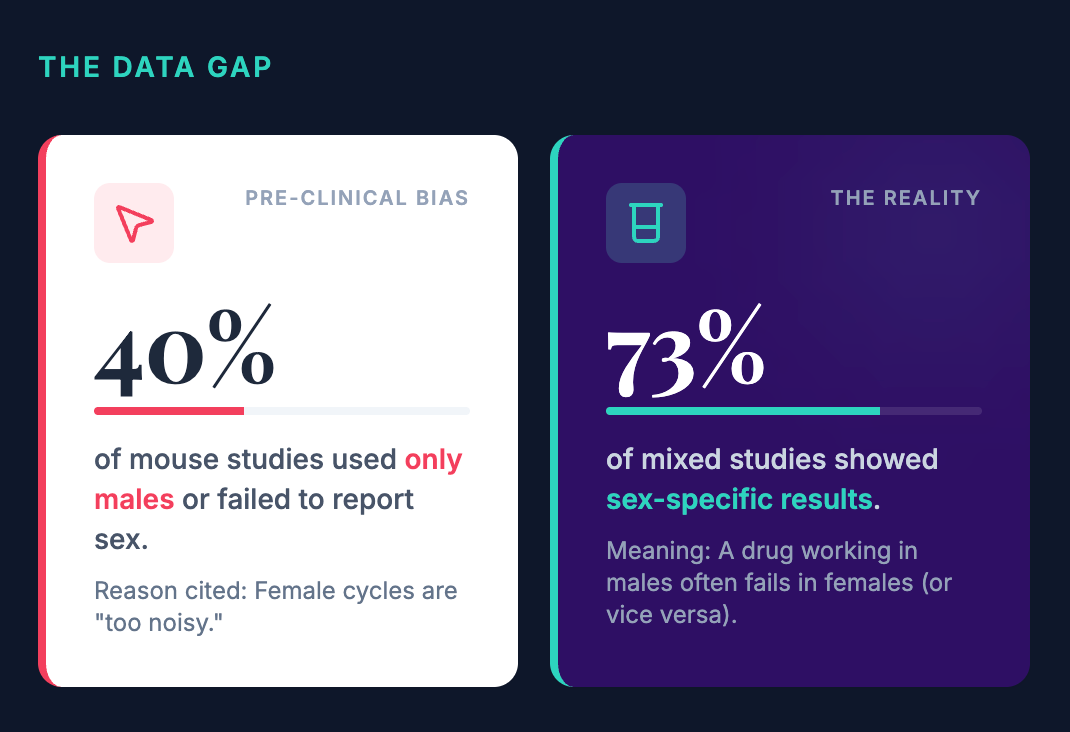
This is a mathematical problem as much as a medical one. It means potential breakthroughs may already exist inside our datasets but are invisible because outcomes have been averaged into noise.
Consider the 2025 preclinical data on OT+A5i (a combination of Oxytocin and an Alk5 inhibitor). It extended remaining lifespan in frail male mice by about 73%, while producing negligible results in females. In a traditional mixed-sex trial, those results would have been averaged together. A miracle drug for one half of the population would have appeared as a mediocre, statistically insignificant drug for the whole.
Ignoring sex differences does not produce neutral science. It produces distorted conclusions.
Female Biology as a Source of Insight
Across species, females consistently live longer. They display stronger immune durability, slower molecular aging, and greater regenerative capacity. Many of the most extreme biological transitions also occur in female physiology. Hormonal cycling. Pregnancy. Menopause. Tissue regeneration such as the endometrium, which repairs and rebuilds roughly four hundred times across a lifetime.
These processes are natural experiments that the longevity field has not yet fully leveraged. They reveal mechanisms of resilience and repair that could inform strategies for everyone:
The Early Warning System: Ovaries age faster than the rest of the body. They are essentially a “canary in the coal mine.” By studying why this specific tissue fails early, we can identify the tipping points for organ failure in the heart or brain decades before they happen.
The Rebound Effect: During pregnancy, biological age markers (like DNA methylation) actually spike. But within months of birth, many women experience a reset where their biological age markers significantly drop. Nature has already built a system for cellular rejuvenation; we just need to learn how to use it.
Why This Matters for the Future of Longevity Science
Precision aging requires accurate baselines. Yet many of the biomarkers used to define “normal aging” were calibrated using largely male or homogeneous cohorts. Cardiovascular risk scores are a prime example: high-sensitivity troponin thresholds frequently miss cardiac events in women because the reference norm is male.
As the longevity field pushes toward earlier detection and AI-integrated tools such as the recently released AlphaGenome, the cost of miscalibration increases. These systems are designed to infer what “normal” looks like from genomic data, but they risk inheriting systematic blind spots if underlying reference datasets are not representative.
We know the depth of this gap from functional genomics. In a 2025 cancer functional-genomics analysis spanning more than 1,200 human cell lines, researchers identified widespread sex differences in gene essentiality. 14 autosomal genes showed consistent sex-biased essentiality across genetic and pharmacologic perturbation screens, indicating that their functional importance differs between male- and female-derived cells in these datasets.
These are not sex-chromosome genes. They are located on autosomes shared by all humans. However, differences in cellular context between the sexes can lead to distinct dependency patterns, meaning female cells may rely more heavily on certain autosomal genes to maintain stability under stress.
This is where calibration becomes consequential. If AI systems such as AlphaGenome are trained primarily on male-biased data, sex-biased gene dependencies risk being averaged into a single baseline. In that scenario, genes that are critical in one biological context may appear only moderately important when assessed across a mixed population.
The downstream risk is not theoretical. Models built on miscalibrated baselines can misestimate safety or efficacy in sex-specific ways. A drug that appears safe or neutral in an averaged model could have unanticipated adverse effects in women, while remaining well tolerated in men. When the reference standard is wrong, every inference layered on top of it becomes less reliable.
A Better Model for the Next Stage of the Longevity Era
If we want to move from hype to impact, we need three strategic shifts:
Sex-stratified measurement Biomarker ranges must reflect sex and hormonal stages, including perimenopause and postmenopause. A “normal” range for a man is not the same for a woman experiencing the metabolic shifts of the menopausal transition.
Bidirectional translation Biological advantages in one sex should inform therapies for the other. This includes studying female immune tolerance to treat chronic inflammation, or male muscle retention to treat frailty in women.
Prevention windows as strategy points Life stages like pregnancy and menopause reveal how the body handles metabolic stress in real-time. These windows can function as models to guide targeted prevention before aging accelerates.
If the goal is extending healthy life for everyone, the science must reflect everyone. Not the average body. The real one.
I totally agree that a longer lifespan does not necessarily equal a longer healthspan. When we overlook women, or conditions that disproportionately affect them with age (like osteoporosis), we risk prolonging ljfe but at what cost to quality?